
Healthcare marketers, especially those in behavioral health and addiction treatment, often carry a kind of inherited skepticism toward Meta. It’s understandable. Behavioral health leads are notoriously difficult to qualify, and in addiction treatment, those leads can come at an extraordinary cost. For years, Meta’s lead forms delivered volume, but not the level of intent an access center needs. Most teams have stories about hours spent calling unreachable submissions or people who had no insurance and never intended to engage.
That reputation came from real experience. Meta’s early lead tools were built for ease, not for the level of qualification healthcare requires. But while many organizations pulled back, the platform continued to evolve. New tools made it possible to verify identity, filter for intent, and connect real patient outcomes back into the algorithm.
In this case study, I walk through how we applied those newer capabilities for a multi-state behavioral health and addiction-treatment organization facing familiar challenges: high CPLs, a high share of unqualified submissions, and pressure to improve acquisition efficiency without sacrificing patient fit.
In four months, we reduced cost-per-new-member by 73% while monthly spend doubled. By the end, Meta was generating new members at a cost 28% lower than paid search. Nothing changed about the service line or the audience. The improvement came from rebuilding the funnel and using Meta’s tools in ways that align with the realities of behavioral health patient intent.
How Meta evolved as a performance channel
Several developments reshaped what was possible on the platform. SMS verification helped eliminate bot traffic by requiring users to validate their phone numbers before form submission. Conditional questions created new opportunities to ask about insurance coverage, treatment preferences, or patient readiness. CRM integrations through the Conversions API made it possible to pass actual conversion data back into the platform so the algorithm could learn what a high-intent patient looked like.
Together, these improvements turned Meta into a more intelligent acquisition channel. But few healthcare organizations had updated their approach. Most continued running lead campaigns the way they had five years earlier.
The client in this case study had a familiar challenge: high lead volume, low conversion rates, and a sales team overwhelmed by unqualified submissions. They were willing to invest in the channel again, but wanted a more predictable, patient-focused system. This became the starting point for the transformation.
A new framework for Meta success
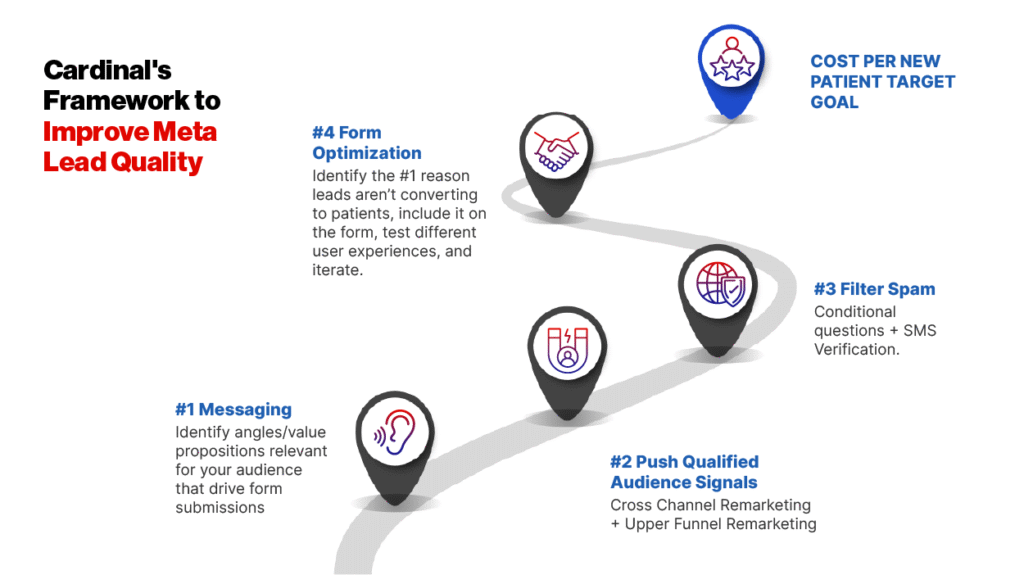
Through repeated testing across behavioral health, physical therapy, vision, and multispecialty groups, Cardinal developed a five-pillar framework that improves both lead quality and patient acquisition efficiency. Each pillar builds on the previous one, creating a step-by-step path from initial creative testing to full-funnel optimization.
Before we began optimizing, we had to understand the root cause of the performance breakdown. The issue wasn’t demand or the service line. It was the structure of the funnel, the lack of qualification signals, and the overwhelming amount of low-intent form submissions.
Healthcare groups looking to strengthen Meta performance can begin with a phased approach:
Pillar 1: Messaging that motivates patients
Before making any technical changes, we focused on what users saw first: the ad creative. Message testing is often undervalued in digital performance programs, particularly in healthcare, where many ads rely on similar templates and language. Yet creative is the mechanism that attracts (or repels) qualified prospects.
Two themes shaped the first round of testing. We compared results-oriented messaging to more supportive, encouraging copy that acknowledged the difficulty of taking the first step toward treatment. Encouragement-focused ads produced a 25% lower cost-per-lead than messages centered on results alone.
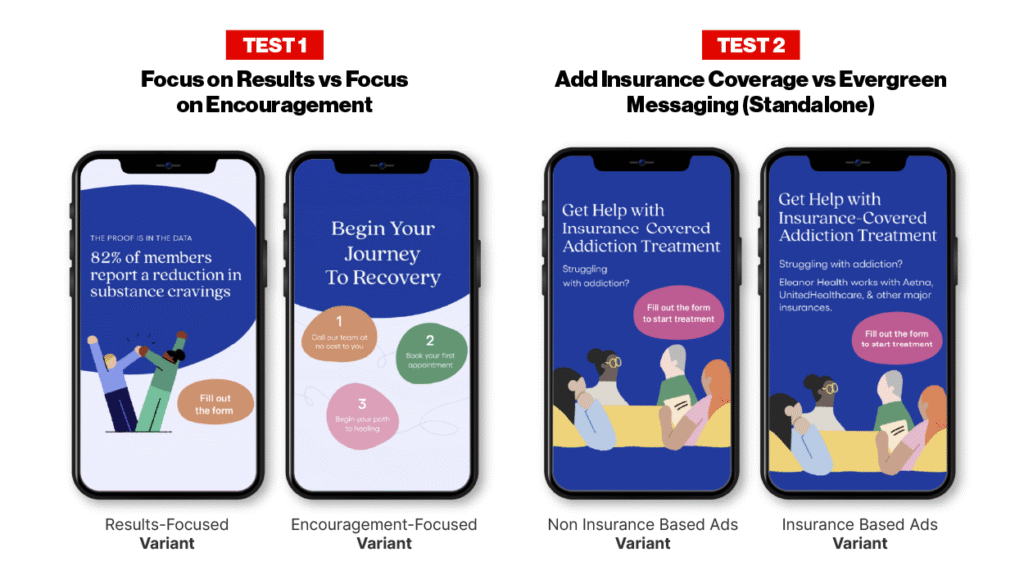
A second test incorporated insurance language. The client’s marketing team had shared an important insight: users with insurance coverage converted at a significantly higher rate. When insurance was mentioned directly in the ad, cost-per-lead improved by 11%. That signal became essential later when optimizing the form itself.
These early tests created a foundation for the rest of the work. Once the most effective messages were identified, budgets were shifted to the ads that produced higher-intent submissions.
Pillar 2: Fueling the algorithm with stronger signals
Meta’s algorithm improves when fed with high-quality audience signals. Instead of pushing lead forms directly to cold audiences, we built a warm-audience approach grounded in engagement.
Video viewers and in-platform engagers became the first targets for lead campaigns. Site visitor and cross-channel remarketing were introduced selectively and only through HIPAA-compliant methods. This ensured that all audience building followed current healthcare regulations and best practices.
This strategy tripled monthly spend while improving lead quality from 17% to 24% qualified. Once the algorithm recognized the behaviors associated with higher-intent users, it delivered ads to people more likely to convert.
The warm-audience structure also created room to scale. As the client expanded budgets, Meta had a larger pool of relevant users to draw from, helping protect efficiency while enabling continued growth.
Pillar 3: Removing spam leads
Although lead quality improved, a significant portion of submissions were still categorized as spam. In March, 57% of unqualified leads were marked as “not a lead/spam.” Users completed the form but provided fake contact information or immediately became unreachable.
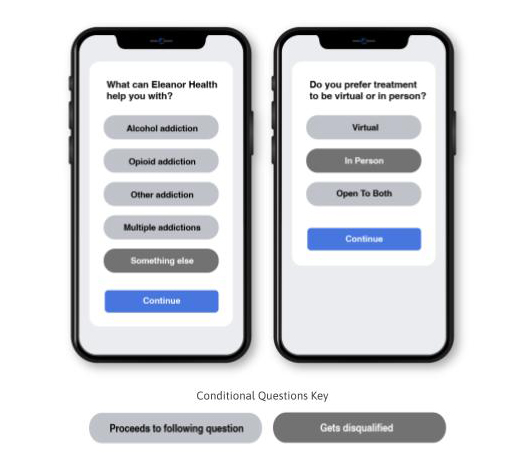
To address this, we added conditional questions that asked about service interest, whether the user preferred virtual or in-person treatment, and willingness to receive a callback. These questions filtered out users who were not ready to engage or had no interest in treatment. After implementing conditional logic, spam fell from 57% to 19% of unqualified leads in one month.
SMS verification was added next. This step required users to validate their phone numbers during form submission, effectively eliminating bot traffic. By June, spam was eliminated.
Removing spam created a clearer picture of true intent. It also saved the access center time and helped identify the next barrier to conversion: insurance coverage.
Pillar 4: Insurance filtering reshaped the economics
With spam removed, the dominant disqualification reason was lack of insurance coverage. Seventy-two percent of unqualified leads fell into this category. We added a conditional question asking users to confirm their insurance, then tested two variations of the form: one displaying a full list of accepted insurance plans, and the other showing plans available only in the user’s state.
The results surprised everyone. The full-list form produced a higher cost-per-lead, but a far stronger cost-per-new-member. The state-specific version looked efficient on the surface, yet conversion from lead to new member was significantly lower. The full list created clarity and helped users self-select earlier, leading to a higher share of qualified submissions.
Adding insurance filtering reduced the cost-per-new-member by 44% month over month. Once the winning form structure was identified, the lower-performing variant was paused, and the budget was shifted to the version that produced better downstream results.
Pillar 5: Optimizing for patient outcomes, not CPL
The final stage of optimization focused on shifting attention away from platform metrics like cost-per-lead and toward business outcomes. When comparing the two insurance form variations, the state-specific version had a much lower CPL. Yet the cost-per-new-member was nearly twice as high as the full-list version. The scheduled rate was also weaker.
This reinforced an important principle for healthcare marketers: CPL is only useful when it correlates with patient acquisition. When it doesn’t, it can obscure the funnel’s true economics. By prioritizing cost-per-new-member and schedule rate, we identified the approach that produced real value for the organization.
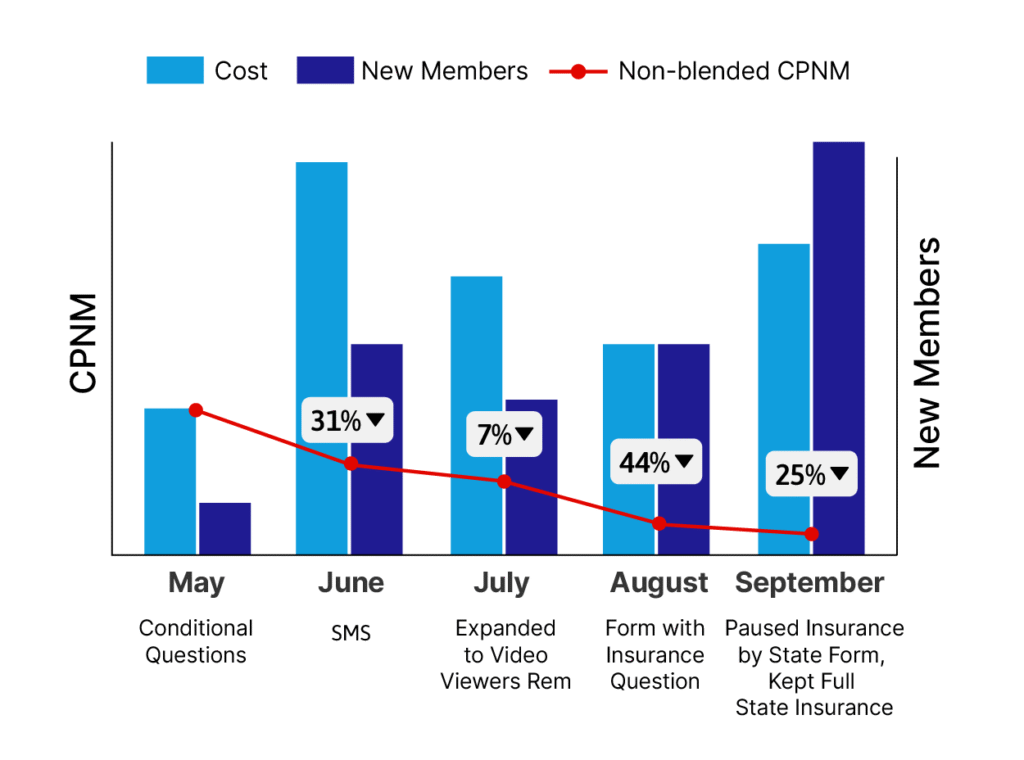
With the optimized form in place, results accelerated. Monthly cost-per-new-member dropped 31% in June, 7% in July, 44% in August, and 25% in September. The client doubled its spend while improving efficiency, and Meta became their most consistent source of new members.
The final results
Four months after beginning the rebuild, the client achieved a 73% reduction in cost-per-new-member. Spam disappeared. Lead quality improved at each stage of the funnel. The algorithm learned to prioritize behaviors associated with treatment readiness. Most notably, Meta surpassed Google paid search, producing new members at a cost 28% lower than search campaigns.
The client continued running Meta as a core acquisition channel and expanded its use of video, remarketing, and CRM integration. The campaign eventually stabilized to a point where daily optimizations became minimal. Meta evolved into a predictable source of new members rather than a source of frustration.
What this means for healthcare marketers
Meta’s evolution is reshaping digital patient acquisition. The platform is no longer defined by high volume and low intent. New tools allow healthcare groups to introduce qualification, verify contact information, and refine audience targeting. When paired with insights from CRM data, Meta becomes capable of identifying and delivering high-intent prospects at scale.
This case study demonstrates what becomes possible when an organization rethinks its approach and invests in rigorous testing. Instead of focusing on lead quantity, the funnel shifted toward patient outcomes. Instead of running campaigns in isolation, creative, audiences, and CRM data worked together. Instead of treating Meta as an awareness channel, the platform became a reliable source of new member growth.
A roadmap for your organization
Healthcare groups looking to strengthen Meta performance can begin with a phased approach:
Phase 1: Build the Foundation
Begin with message and creative testing. Identify which themes consistently attract higher-intent users, not just clicks or cheap leads. This often includes testing encouragement-focused copy, value props, and insurance callouts. At the same time, run top-of-funnel video or educational campaigns to create early warm audiences that will later fuel retargeting.
Phase 2: Strengthen Audience Signals
Shift from cold audiences to warm pools, based on engagement signals like video views. And where appropriate, use site visitors and cross-channel remarketing audiences built through HIPAA-compliant methods, such as with a customer data platform (CDP) or server-side tracking. This gives Meta stronger behavioral signals and sets the stage for more efficient lower-funnel performance.
Related: If you want a deeper breakdown of Meta’s privacy requirements and what’s allowed, explore this article on Meta’s data restrictions.
Phase 3: Qualify and Verify
Add the form elements that filter out noise. Include conditional questions aligned to your operational requirements: treatment interest, preferred modality, callback readiness, and insurance, if relevant. Turn on SMS verification to eliminate fake submissions. This combination reduces spam, clarifies true intent, and saves your access center time.
Phase 4: Use CRM Data to Guide Optimization
Look closely at why leads fail to convert. If lack of insurance is the primary issue, add or refine your insurance questions. If location or readiness is the barrier, adjust the form accordingly. Test variations, but evaluate them against cost-per-new-patient rather than CPL. CRM insights should drive both creative and form structure.
Phase 5: Scale and Sustain
Once you see which form experiences and audience combinations produce real patients, scale gradually. Maintain creative diversity, continue feeding warm audiences, and revisit CRM data regularly to ensure alignment with real-world qualification patterns. As Meta accumulates conversion data, performance stabilizes and the system becomes easier to manage.
A new chapter for Meta in healthcare
Meta is becoming an essential part of the healthcare acquisition mix. It reaches audiences that search cannot and surfaces patients earlier in their journey. When built thoughtfully, it reduces blended acquisition costs and creates a more efficient path to growth.
For years, Meta was seen as a playground for low-intent leads. That chapter is ending. A smarter funnel reveals what the platform can truly deliver. And based on what we saw in this case study, I expect more healthcare groups will start to rethink how Meta fits into their acquisition mix.
Want a deeper walkthrough of this strategy? Watch this recording from the Scaling Up stage, where I break down the full case study.