

Most healthcare marketing teams are running paid media campaigns that seem to be working. The leads are coming in. The cost-per-lead looks reasonable. But marketing is reporting good numbers while the business isn’t seeing an increase in new patients. And the root cause is almost always the same: poor conversion signal strategy.
Table of Contents
This is a foundational issue in how paid media strategy is set up and measured. The signals being fed to the algorithm often have little connection to what a real patient acquisition actually looks like, and the algorithm dutifully optimizes for exactly what it’s been told to find.
Conversion signals have become the most crucial component of optimizing the algorithms to work in your favor. In Google Ads, conversion signal optimization and bid strategy account for 50% of performance impact, as our VP of Paid Media, Evan Ilgenfritz, loves to remind us. And as ad platforms lean further into machine learning and automation, that impact is only growing.
So how do you fix it? The short answer is that you need to climb the conversion signal staircase and incorporate it into your bidding strategy. But since that short answer doesn’t tell you anything about how you’d go about doing it—let alone do it in a HIPAA-compliant manner while avoiding common mistakes—this guide will give you a clearer picture of what conversion signal optimization strategy looks like and how to get there.
1) Why do conversion signals drive paid media performance?
How the algorithm actually works
Ad platform algorithms, whether it’s Google, Meta, or whoever, all work the same way:
- You feed them examples of your successful conversions
- The algorithm analyzes the data
- It goes out and finds you more users who look like those examples
It’s basically pattern matching. The idea is to feed in lots of data that tells the algorithm “here’s a bunch of examples of what users that convert look like”, and then the algorithm says, “great, I’ll find you an audience that looks like that.” The examples you feed the algorithm are your conversion signals and the primary factor in determining which audience sees your ads.
Why are conversion signals so important now?
Even up until a few years ago, you could largely build your own audience with exact keywords and lots of precisely targeted campaigns. But we’ve seen a major shift in the ad platforms towards automated campaign management and smart bidding. Google Demand Gen, Google PMAX, and now AI Max. Even Meta Advantage+. The major ad platforms are now asking you to run a few broader campaigns and let the algorithm create the audience based on your conversion signals. That means your signal quality matters more than ever.
And this is increasingly not optional. The whole industry is shifting towards a more AI-first automated ecosystem where marketers have less manual control. As Ruchi Patel, Group Media Director, noted on the Ignite podcast:
“The emphasis is very heavily on: Let *us* figure out who the best audience is; you just tell us who has converted in the past.”
That’s modern paid media optimization in a nutshell. No more manual control over targeting and bidding decisions. The algorithm is in control and your control is largely reduced to two inputs that you feed it:
- Your creative
- Your conversion signals
From there, Google or Meta will go out and find that audience for you, based on whatever you told it was the primary conversion action. Which sounds convenient, but leads to one major problem:
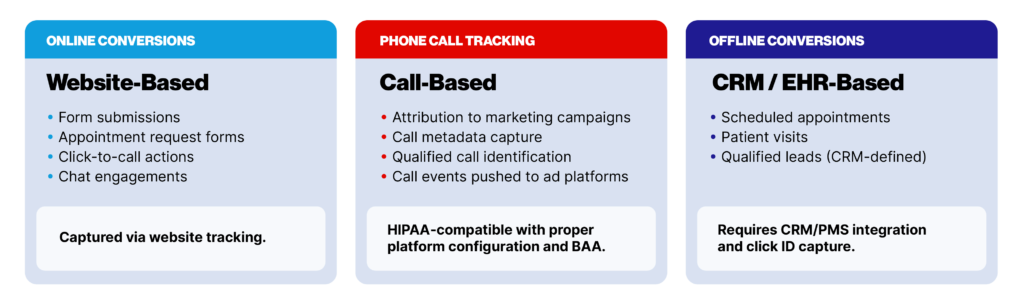
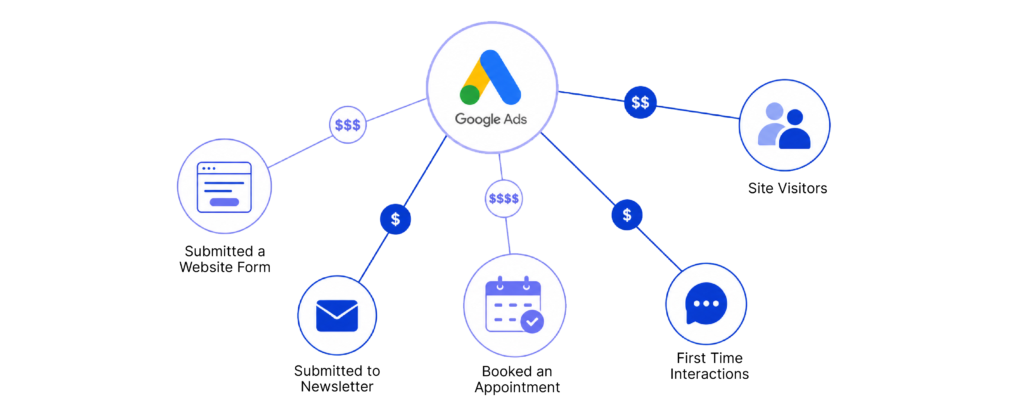
Types of signals
Conversion signals fall into three broad categories, each reflecting a different stage of the patient journey and a different level of integration complexity to capture and activate.
Poor conversion signals kill campaigns
Because the algorithms rely so heavily on the conversion signals, there’s a very real “garbage in, garbage out” problem. The algorithm doesn’t understand value. It only knows what you tell it. So if you set up a campaign and train it on form fills as your primary conversion signal, you’re going to be optimizing for form fills. That means the algorithm is going to learn to bring in as many people as possible who seem likely to fill out a form.
But most of those people will never become patients. Rather than teaching the algorithm to focus on likely patients, you’ve told it to maximize form fills. And even if it does a great job at that, it’s not necessarily driving any new bookings. This KPI mismatch is often a source of problems because ad platforms will report great performance in meeting those conversion-signal goals, while the C-suite still sees a lack of new patients coming through the doors.
We see this all the time in paid media audits. Campaigns that look like they’re performing well but still don’t seem to be driving bookings. Those campaigns are meeting the goal they were given… but that goal was based on a weak conversion signal that wasn’t tied to actual business outcomes.
Conversion signals matter.
2) The conversion signal staircase
The signal spectrum
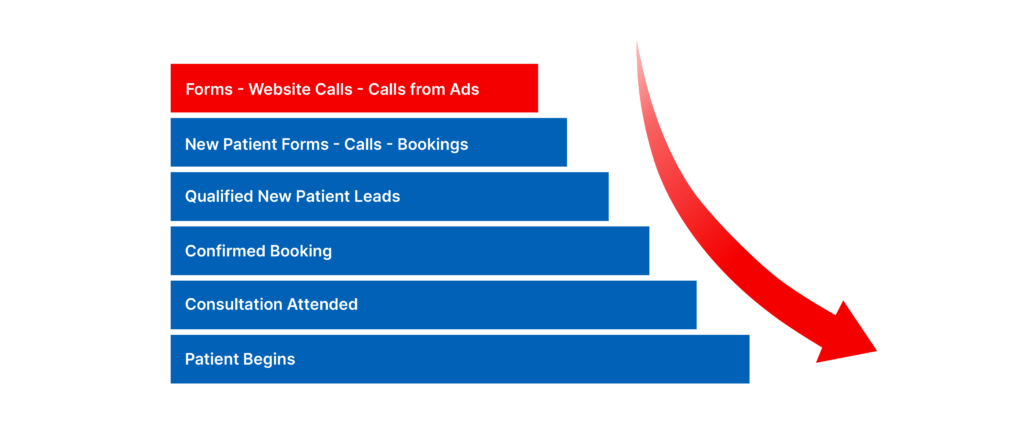
Conversion signals span a spectrum along the patient journey, from the weakest early in the journey to the strongest near actual business outcomes.
Weakest:
- Website interactions (clicks, page views)
- Form submissions, website calls, calls from ads
- Qualified leads
- Booked appointments
- Kept appointments
- New patients
Deepest:
The deeper the signal, the more meaningful the conversion metric you can feed the algorithm and optimize towards. But using those deeper signals has a cost. Two costs, actually: Volume and latency.
- Volume is important because if you’re only getting 7 new patients per month from your campaign, that’s not a statistically significant dataset for the algorithm to optimize. We’ll address the volume problem in more depth later.
- Latency is an issue because measurement becomes much more complicated if it takes two weeks for any patients to actually show up.
Keeping both of these issues in mind, leaping directly to patients as your conversion signal isn’t always the best option. But you generally do want as deep a signal as you can support.
Your conversion signal sets your performance ceiling
The best result you can expect from your campaign is for the algorithm to succeed at finding the audience you asked it to find. That’s how you’ve defined success. The signal you optimize toward is an instruction to the algorithm about what a valuable user looks like—and those are the users the algorithm will find. So if your signal was based on clicks, you can expect a lot of clicks from your campaign, but might not see any impact on business outcome.
Ideally, you want a signal that’s as close to the business outcome as possible. As Scott Cameron, Group Media Director, put it on the Ignite podcast:
“We can take something like a shallow conversion signal, and if we can move that further along to tie that towards real business outcomes, we see complete changes in performance. That’s really been the biggest shift—being able to move towards those better signals.”
The closer you get to business outcomes, the more precise the signal to improve campaign performance. But that doesn’t mean you can immediately start using the strongest possible signal. What you’re looking for is progress.
Progress over perfection
A smart conversion signal strategy requires considering both volume and latency when asking how deep you can currently go on the signal spectrum. But you should always have an eye towards improvement.
In short, you want to:
- Identify the deepest conversion signal you have the volume + measurement to support
- Optimize towards that conversion signal
- Build a roadmap for how to get to the next achievable step
As Evan Ilgenfritz puts it:
“The expectation is not just accepting the current state—it’s challenging what the next step down the funnel looks like and how we get there.”
We like to call this the “Conversion Signal Staircase”. You start as deep as your data allows, but then you’re constantly pushing towards deeper signals. And that’s going to be limited by your infrastructure and integration because most healthcare organizations can’t currently pass kept appointment or new patient data to ad platforms. That kind of integration is especially complex in the current privacy landscape and requires connecting your EHR or PMS through a HIPAA-compliant martech stack.
3) The HIPAA problem—and how to solve it
Healthcare marketing is harder
Measurement in healthcare presents unique challenges that other industries don’t face. If you’re doing e-commerce, retail, or CPG marketing and you want to connect a conversion to an ad platform, the pixel captures everything, the platform records the conversion, and the algorithm ingests it to optimize. Easy, right?
In healthcare, HIPAA makes that a huge legal risk. Any data linking a person’s identity to a health condition or care-seeking behavior is considered protected health information (PHI), and transmitting that data exposes you to liability. And yes, that includes when your Google tags and Meta pixels transmit it automatically.
Thankfully, we have the marketing technology to anonymize patient data with a tech stack of purpose-built tools:
The 3 pillars of compliant martech
Privacy platforms and CDPs: Tools like Freshpaint, Tealium, and Ours Privacy sit between the website and ad platforms, stripping PHI before data is transmitted.
Server-side tracking: Routes data through a secure server you control to be anonymized before anything is sent to third-party platforms. GTM Server-Side (hosted via Stape.io or Google Cloud) or Freshpaint (with managed hosting) are options.
Call tracking tools: Platforms like Liine and Patient Prism (premium-tier options with AI booking classification), as well as Invoca, CallRail, and Call Tracking Metrics capture call outcomes (booked appointment, qualified inquiry, unqualified call) and can pass those classified signals back to ad platforms without transmitting patient identity.
How to pass back offline conversion data
Once you’ve got your compliant martech stack in place, the next step is getting deeper conversion data—booked appointments, kept appointments, new patients—out of your EHR or CRM and back into Google Ads. This is where most healthcare organizations stall, and where the biggest performance gains are waiting.
There are three paths to get there, in ascending order of reliability:
1) Manual matchback
Your analytics team manually matches appointment data back to ad clicks using a shared identifier like a phone number. It’s the highest-effort, lowest-fidelity option—prone to delay and human error—but better than nothing when other integrations aren’t available yet.
2) Offline conversion file upload
Appointment or patient data is exported from your CRM or EHR, de-identified, and uploaded to Google Ads on a set cadence. For this to work, the file needs to contain specific fields Google requires:
- Google Click ID (GCLID): the exact identifier from the original ad click—case sensitive, cannot be truncated
- Conversion name: must match the conversion action name in Google Ads exactly, including capitalization and spacing
- Conversion time: timestamp of when the conversion occurred, in UTC format (yyyy-MM-dd HH:mm:ss +0000)
- Conversion value: dollar amount, required if you’re using Target ROAS bidding
- Currency code: ISO 4217 format (e.g., USD), required if a value is set
- Order ID: a unique identifier recommended for deduplication—prevents the same appointment from being counted twice
A manual CSV upload is a valid starting point, but not a sustainable long-term setup. Every step in that human chain—generating the export, scheduling the upload, checking for errors—introduces delay and risk. Google recommends uploading at least daily, because stale conversion data directly degrades Smart Bidding performance. The model relies on recent signals to make real-time bid adjustments; weekly uploads mean the algorithm is operating on data that’s up to seven days old.
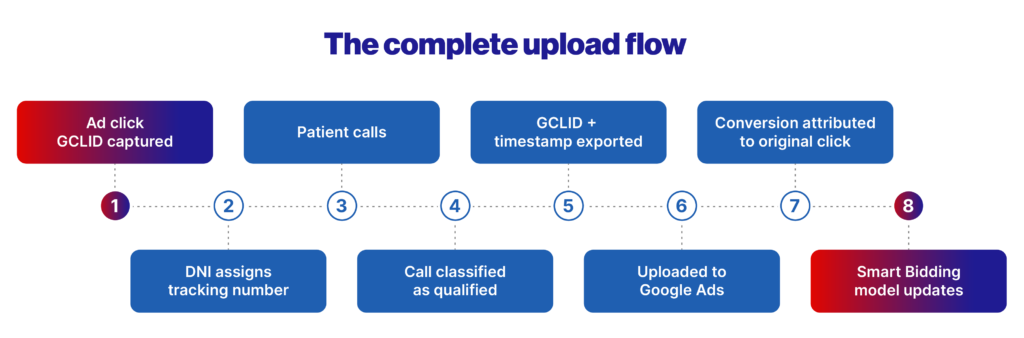
3) Automated GCLID passback
The target state. When a patient clicks an ad, Google generates a GCLID. Your call tracking platform, form tool, or online scheduler captures that GCLID, strips PHI, and passes it into your CRM or EHR. An ETL tool like Funnel.io then pulls that data and pushes it back into Google Ads as an offline conversion action—automatically, every day. Most major call tracking platforms have native Google Ads API integrations that make this possible without manual intervention.
If you’re using automated upload, verify it’s actually working: Google Ads → Tools → Conversions → Upload History. A connected integration that is silently failing is the worst-case scenario—it looks like it’s working while your campaigns are optimizing on incomplete data.
How to structure your conversion actions
Each call classification level should be its own conversion action in Google Ads. Mixing call types into a single action means you lose visibility into performance by call type and can’t assign different bid strategy weights to each one.
A standard setup looks like this:
- Qualified call: provides volume signal to the algorithm
- Booked appointment: provides quality signal; weight this higher via conversion values if you’re using Target ROAS
- High-value service inquiry (optional): useful for multi-specialty organizations where service lines carry meaningfully different patient values
Include both qualified calls and booked appointments in your Conversions column for Smart Bidding. The combination gives the algorithm enough volume to learn from while still orienting it toward the outcomes that matter.
One final note: offline conversion upload is infrastructure, not a one-time setup. It requires ongoing monitoring, deduplication checks, and daily verification. Automate everything you can—and then monitor what the automation is actually doing.
Workarounds when direct integration isn’t possible
Offline conversion data is too valuable to ignore, so even if automated GCLID passback isn’t an option, don’t just throw up your hands and say, “Well, I guess we can’t track that.” You definitely want to track those deeper offline conversion metrics, so it’s worth talking with your agency or internal IT stakeholders and figuring out what options you have.
For example, most of our clients use online schedulers. And because those schedulers tend to live in an iframe or off-site on an entirely separate third-party page, the standard tracking setup does not work. But we still want to track those booked appointments. So we have three standard workarounds that we tend to suggest, in ascending order of effort:
1) Native integrations
Check whether the scheduler natively integrates with a martech tool you’re already using. For example, NexHealth works with GA4. ZocDoc integrates with Liine. So if you use Liine, and you’re scheduling through ZocDoc, you can use that integration to send the online bookings through Liine and then push that back to the ad platforms. This is the easiest option when it’s available.
2) Embedded scripts
By placing Google Tag Manager code or other scripts inside the scheduler, you can push events back to the data layer. Requires slightly more effort, but placing a GTM container inside the scheduler lets you push booking events back to Google Ads via the data layer.
3) Thank-you page redirect
Ask the client or vendor to redirect back to an on-site thank-you page after booking so you can fire a conversion pixel. Then you can append query parameters to differentiate between new patient and existing patient appointments, or even make entirely separate thank-you pages. But you want to be able to differentiate so you can fire those pixels as different conversion actions with different assigned values.
As Chief Growth Officer Lauren Leone says about driving results:
“At least ask the organization with the tech you’re using for online scheduling whether after it’s submitted, [it can redirect] and perhaps you can capture just a hit on a thank you URL. That’s always something we like to toss out there as a nice-to-have, if it’s possible.”
In short, whenever you’re being told, “Oh, we can’t track offline conversions,” it’s worth asking what options you might not have explored. Deeper signals await you.
4) The volume problem
Why the deepest signals aren’t always the best
Signal depth is incredibly important, but it’s not the only factor to consider. The algorithm also requires a minimum volume of conversion events to learn effectively. So you don’t want to go so far down the funnel that you’re trying to base your whole campaign strategy off of seven new patients. That’s just not enough.
You want 20-30 conversions per campaign per month, minimum. The exact number varies by campaign, but that’s generally the threshold. Obviously more is better so the algorithms have even more information to work with. But 20-30 monthly conversions is the bare minimum.
Below that, you’re not giving the algorithm sufficient data to identify patterns, and performance is likely to become erratic or stall out entirely.
We see this happen all the time. We recently audited a prospect and found that only 4 of the 20 campaigns they were running were meeting the minimum conversion volume threshold. Which means a full 80% of their campaigns were basically flying half-blind because the algorithms didn’t have enough data to optimize effectively.
In those instances, you should use a shallower signal in order to get enough volume.
Signal volume issues hit hardest for high-acuity
The volume issue is especially important for high-acuity providers (oncology, cardiology, neurology, etc.)
- Patient volume is inherently lower for high-acuity
- Practices may only see 20-30 new patients per month overall
- Optimizing for patients starves algorithms of data points. Thin signals bring poor performance.
Campaign-level conversion goals can help
Conveniently, Google offers a great option to address some of these volume issues through campaign-level conversion goals. This lets you set different campaigns to optimize toward different signals simultaneously, based on the volume each one is driving.
So if you’ve got a dozen campaigns all running simultaneously, you can look at the new patient volume actually being driven by each one and then set your conversion goals accordingly:
- High-volume campaigns optimize toward kept appointments (for maximum signal depth)
- Mid-volume campaigns optimize toward booked appointments (balancing depth and volume)
- Lower-volume campaigns optimize toward qualified leads (ensuring sufficient signal volume)
That way every campaign gets the deepest signal it still has enough data to learn from, and you go down the staircase based on available volume. We’ve had success testing this approach for our clients, and it’s been a great way to push toward quality where volume supports it, while still keeping the broader campaign structure healthy by ensuring there’s always enough conversions for the algorithms to function smoothly.
The other big way to handle this is value-based bidding.
5) Value-based bidding: bridging quality and volume
What value-based bidding is and why it matters
Value-based bidding lets you optimize for the expected value of various conversion actions, rather than just lumping everything together. This lets you use multiple conversion signals in a single campaign. You assign different monetary values to conversion actions and then use a bid strategy that optimizes for higher-value outcomes across the entire campaign. Maximize Conversion Value is an obvious choice. Target ROAS also works.
Instead of just optimizing towards one conversion action and ignoring everything outside the sweet spot, you can include multiple signals. The algorithm then has a better volume of signals to ingest, looks at how you’ve weighted them, and optimizes towards the most valuable outcome.
But using multiple conversion signals only works if you weight the values and then tell Google to optimize for value. Otherwise, you’re optimizing for conversion volume and telling the algorithm that every conversion signal is equal. Which they’re not. A call is not worth the same as a booking. We all know that. So the purpose of weighted conversion value is to make sure that Google knows it too.
As Scott Cameron put it on the Ignite podcast:
“Are we teaching the algorithm that a click is the same value to us as somebody who has visited the site multiple sessions and gone to the insurance verification page? It’s probably not. We want to make sure that the algorithm understands the value of those events and it’s cleaner.”
How to determine conversion values
The best way to calculate the conversion value is to work backward from your new-patient value. So let’s say a new patient is worth $1000. (You could plug in your actual patient LTV here, but since we’re just looking for relative conversion values for Google to weigh, using $1000 is going to make the math easier.)
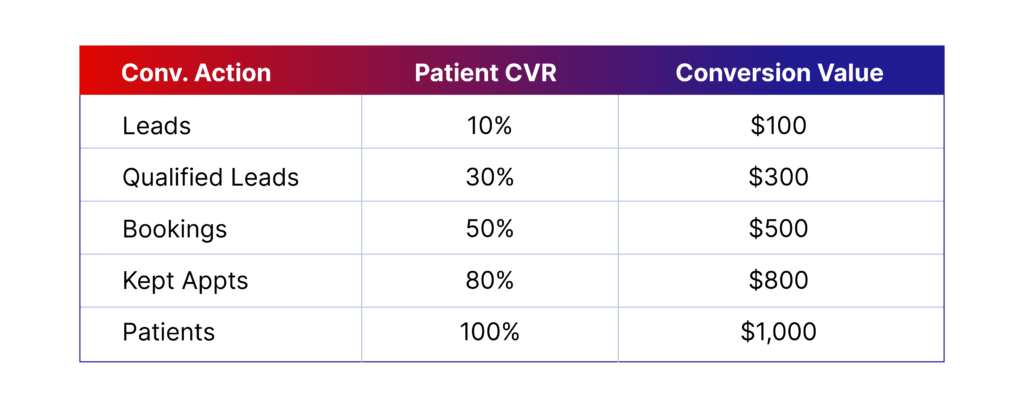
So we tell Google that a new patient has a $1000 conversion value. Then we look at leads: What percentage of leads actually become new patients? If 10% of leads become patients, a lead is worth $100. (Note that you will need your actual conversion rates for all the percentages—if your CRM data tells you 7.2% of your leads become new patients, then you multiply that percentage by the new patient value of $1000 and get a value of $72 per lead.)
Then you just go down the signal list and plug in your patient conversion rates. In our example, if 30% of qualified leads become patients, a qualified lead is worth $300. If 50% of bookings become patients, a booking is worth $500. As long as you have the percentages right, the dollar value doesn’t really matter because it’s just a way to tell Google the relative weight of conversion value. If 10% of your leads become patients, then what Google needs to know is that a patient is worth 10x a lead. You can call a patient $1000 and a lead $100, or call a patient 10 and a lead 1. The key is the relative weighting.
Also worth noting: you can break this down by appointment type if you offer widely varying services. If you’re running a campaign for a dentist who does general dentistry and also orthodontics, you might know that a kept ortho appointment is going to be worth 10x a kept general dentistry appointment. So you want to separate those conversion signals. And then weight them appropriately so that Google also knows one is 10x more valuable when it’s trying to maximize your value.
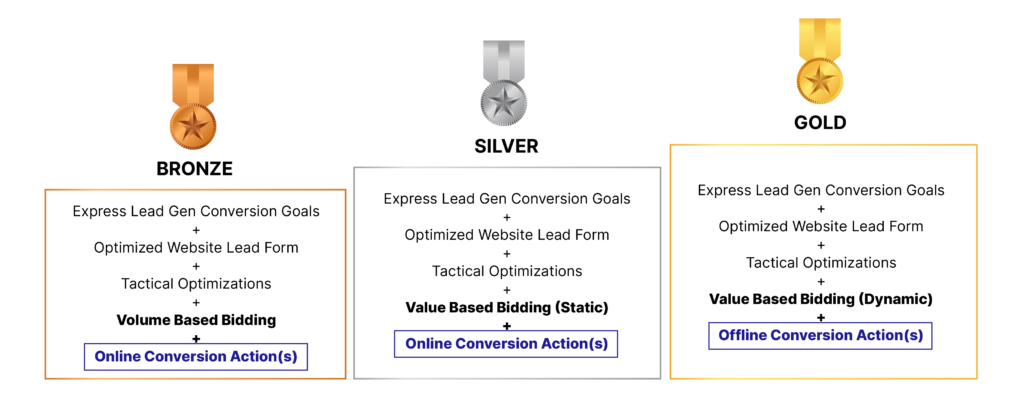
The Bronze/Silver/Gold framework
Even back in 2025, Google was already saying that to be at that top level really requires value-based bidding as well as accounting for offline conversion actions.
New Booked Appointments remain one of the strongest conversion signals you can optimize toward. But online booking data is often inaccurate. We’ve had clients where we found online booking tracking was overcounting by 60%. People went to book, then canceled and booked with someone else, and Google was still optimizing for those original bookings. That’s why offline conversion actions like Kept Appointments are the target state: they reflect what actually happened, not just what was scheduled.
Google’s own maturity framework gives us a useful way to identify where you currently are in terms of sophistication in conversion signals and bidding strategies.
- Bronze: Volume-based bidding with online conversion actions only—(where most orgs start)
- Silver: Static value-based bidding with online conversion actions—(a big step up in signal quality)
- Gold: Dynamic value-based bidding with offline conversion actions like kept appointments—(the target state for mature programs)
And just like with the signals themselves, your goal is to work your way down the staircase. Most healthcare orgs are not coming in with the infrastructure to be at Gold level immediately. Usually you’re starting at Bronze. You’re looking at what it’s going to take to get to the next step, both in terms of bidding and conversion actions, and putting together a roadmap so you can incrementally start building towards a more mature signal strategy.
6) Testing conversion signals without breaking performance
Now that you understand the many benefits of value-based bidding and deeper conversion signals, it may be tempting to go in tomorrow and switch all your accounts over to the best signal strategy you can. And I’d like to encourage you NOT to do that.
Changing conversion configuration is not a frictionless action. It has a pretty significant impact on the algorithm, which can take 2-4 weeks to adapt to a new conversion setup and learn how to optimize for it. And in the meantime, performance can suffer. Not so much that it still isn’t worth doing… but enough that you don’t want to do it to your entire business, especially repeatedly.
That’s why switching your conversion strategy at an account level is risky. You’re not only disrupting all of your campaigns at once, but you can’t even be sure the new setup is what’s actually the best for you. Hard to isolate what’s affecting performance when you’ve just shifted everything.
A smarter way to go about it is to test the impact before you change everything.
The right way to test
Campaign-level conversion goals are the best way to test the impact of switching signal strategy on a subset of campaigns. You set up an experiment using the new set of conversion actions, against a control using the existing set of conversion actions, and see how they perform differently.
Google’s Campaign Experiments tool makes this easy. It gives you a structured A/B testing environment for conversion and bid strategy changes. So you can run those experiments and then get that performance comparison between your control group and your test group to see what works before committing account-wide.
And even when you’ve finished an experiment on one campaign, you may not want to shift your whole account at once. Even if most campaigns thrive with Target ROAS bidding, you might find that you have one or two campaigns that actually work better with Target CPA. But you won’t find that out if you don’t test at the campaign level.
Two important caveats before you start testing
1) Make sure you have enough volume.
If you’re running a campaign experiment where you’re A/B testing, don’t forget that each half still needs sufficient volume for the algorithm to optimize. So if 30 conversions was the minimum volume before, now it’s 60. And the higher the volume, the faster the algorithm can re-learn, and the shorter the period of negative disruption. So counter-intuitively, testing your highest-volume campaigns first can actually cause less disruption.
2) Make sure you have enough time.
You need to give the algorithm enough time to optimize for the new value-based bidding—and that time should start at least a month BEFORE your experiment. If you’re shifting to value-based bidding for the first time, the algorithm lacks historical data, a crucial input. So once you’ve nailed down the correct relative conversion values, plug them in and let it marinate for 4+ weeks before you start using value-based bidding. And then a couple of weeks after, so the algorithm has time to adapt.
This is also why it’s important to find your actual conversion percentages so you can input the right conversion values the first time around. Every time you change the target, the algorithm is going to take weeks to catch up. So test in areas of the account where you have sufficient volume, be deliberate with your decisions, and give the algorithm enough time on both ends to adapt to the new values before you start drawing conclusions.
Conclusion: Where to start
What steps can you take today to start optimizing your conversion signals?
- Conduct an honest audit of your current conversion setup. What signals are you actually optimizing toward today, and how far are they from a real patient outcome?
- Identify the gap between your current signal and the next achievable step. Often this is less about technology and more about pushing for the right martech integrations.
- Prioritize the compliance infrastructure first. Without a HIPAA-compliant data pathway, deeper signals can’t be used safely regardless of how valuable they are.
The goal is always to optimize toward the best signal you can get enough volume from, continuing to move down the funnel as your data infrastructure matures. And of course, if you need any more personalized help with your conversion signal strategy, please don’t hesitate to drop us a line.